Approximately one month after hospital discharge, 86 COVID-19 patients underwent physical examination, arterial blood gas (ABG) analysis, pulmonary function tests (PFTs), and six-minute walk test (6MWT).
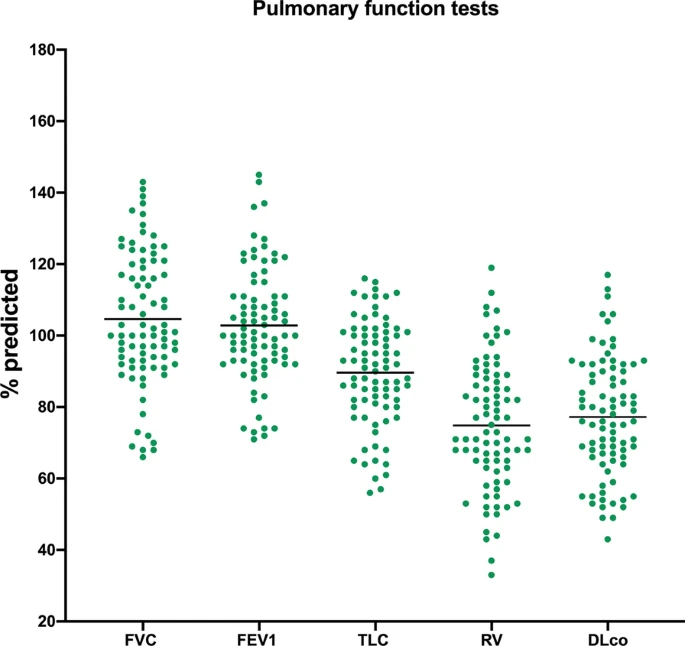
Patients were also asked to quantify the severity of dyspnoea and cough before, during, and after hospitalization using a visual analogic scale (VAS). Seventy-six subjects with ABG during hospitalization were stratified in three groups according to their worst p/F values: above 300 (n = 38), between 200 and 300 (n = 30) and below 200 (n = 20).On PFTs, lung volumes were overall preserved yet, mean percent predicted residual volume was slightly reduced (74.8 ± 18.1%). Percent predicted diffusing capacity for carbon monoxide (DLCO) was also mildly reduced (77.2 ± 16.5%). Patients reported residual breathlessness at the time of the visit (VAS 19.8, p < 0.001). Patients with p/F below 200 during hospitalization had lower percent predicted forced vital capacity (p = 0.005), lower percent predicted total lung capacity (p = 0.012), lower DLCO (p < 0.001) and shorter 6MWT distance (p = 0.004) than patients with higher p/F.
Approximately one month after hospital discharge, patients with COVID-19 can have residual respiratory impairment, including lower exercise tolerance. The extent of this impairment seems to correlate with the severity of respiratory failure during hospitalization.
No comments:
Post a Comment