
Ellis, A.K., Cook, V., Keith, P.K. et al. Allergy Asthma Clin Immunol 20, 45 (2024). https://doi.org/10.1186/s13223-024-00899-3
Abstract
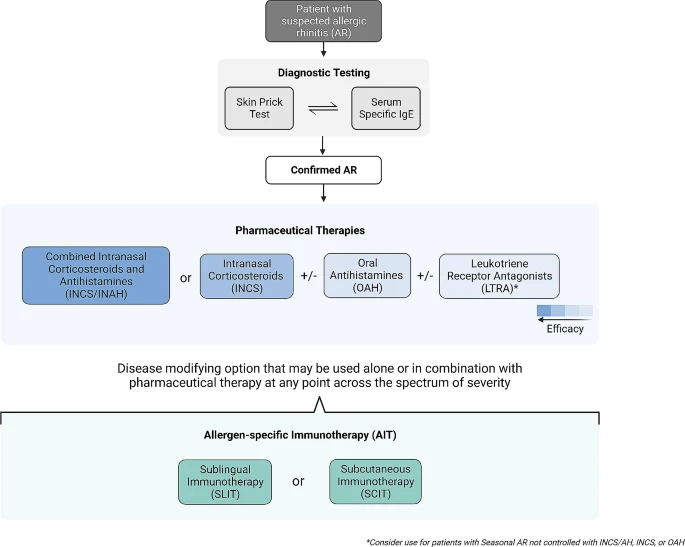 |
| A stepwise algorithm for the diagnosis and treatment of allergic rhinitis. |
Abstract
|
| A stepwise algorithm for the diagnosis and treatment of allergic rhinitis. |
No comments:
Post a Comment