Grenier PA, Brun AL, Longchampt E, Lipski M, Mellot F, Catherinot E. Eur Radiol. 2024 Jun;34(6):4142-4154. doi: 10.1007/s00330-023-10334-7.
Abstract
Our objective in this review is to familiarize radiologists with the spectrum of initial and progressive CT manifestations of pulmonary complications observed in adult patients with primary immunodeficiency diseases, including primary antibody deficiency (PAD), hyper-IgE syndrome (HIES), and chronic granulomatous disease (CGD).
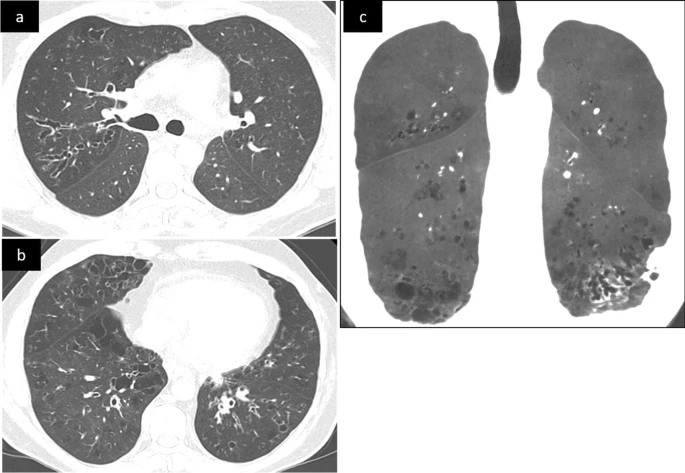 |
| Unenhanced CT scan in a 35-year-old patient with common variable immunodeficiency (CVID) |
In patients with PAD, recurrent pulmonary infections may lead to airway remodeling with bronchial wall-thickening, bronchiectasis, mucus-plugging, mosaic perfusion, and expiratory air-trapping. Interstitial lung disease associates pulmonary lymphoid hyperplasia, granulomatous inflammation, and organizing pneumonia and is called granulomatous-lymphocytic interstitial lung disease (GLILD). The CT features of GLILD are solid and semi-solid pulmonary nodules and areas of air space consolidation, reticular opacities, and lymphadenopathy. These features may overlap those of mucosa-associated lymphoid tissue (MALT) lymphoma, justifying biopsies. In patients with HIES, particularly the autosomal dominant type (Job syndrome), recurrent pyogenic infections lead to permanent lung damage. Secondary infections with aspergillus species develop in pre-existing pneumatocele and bronchiectasis areas, leading to chronic airway infection. The complete spectrum of CT pulmonary aspergillosis may be seen including aspergillomas, chronic cavitary pulmonary aspergillosis, allergic bronchopulmonary aspergillosis (ABPA)-like pattern, mixed pattern, and invasive. Patients with CGD present with recurrent bacterial and fungal infections leading to parenchymal scarring, traction bronchiectasis, cicatricial emphysema, airway remodeling, and mosaicism. Invasive aspergillosis, the major cause of mortality, manifests as single or multiple nodules, areas of airspace consolidation that may be complicated by abscess, empyema, or contiguous extension to the pleura or chest wall. CLINICAL RELEVANCE STATEMENT: Awareness of the imaging findings spectrum of pulmonary complications that can occur in adult patients with primary immunodeficiency diseases is important to minimize diagnostic delay and improve patient outcomes. KEY POINTS: • Unexplained bronchiectasis, associated or not with CT findings of obliterative bronchiolitis, should evoke a potential diagnosis of primary autoantibody deficiency. • The CT evidence of various patterns of aspergillosis developed in severe bronchiectasis or pneumatocele in a young adult characterizes the pulmonary complications of hyper-IgE syndrome. • In patients with chronic granulomatous disease, invasive aspergillosis is relatively frequent, often asymptomatic, and sometimes mimicking or associated with non-infectious inflammatory pulmonary lesions.PDF
No comments:
Post a Comment