
What is Known: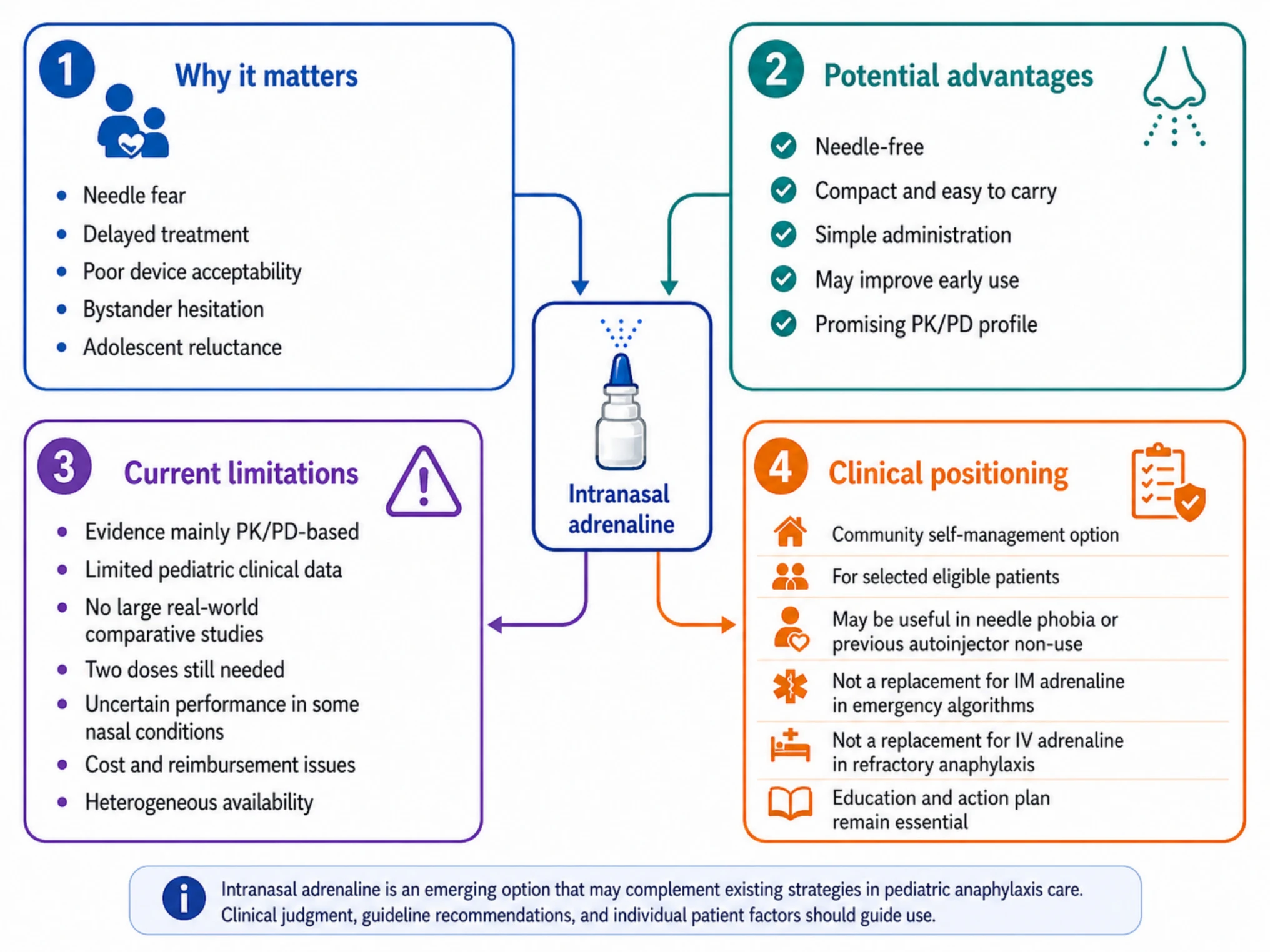
Intranasal adrenaline in pediatric self-management: promise and limits.
• Intramuscular adrenaline is the first-line treatment for anaphylaxis and should not be delayed.
• Food is the leading trigger in children, while drugs, venom, and cofactors become more relevant with age.
What is New:
• Intranasal adrenaline is a promising needle-free option, but pediatric evidence remains limited.
• Omalizumab and oral immunotherapy may reduce risk but do not replace emergency preparedness.
Abstract
Anaphylaxis is a time-critical, potentially fatal systemic hypersensitivity reaction. This narrative review summarizes recent advances in the diagnosis and management of anaphylaxis in children and adolescents, with emphasis on new diagnostic frameworks, improved self-management strategies, intranasal adrenaline, and disease-modifying therapies.
A narrative review was conducted using PubMed and MEDLINE, focusing on articles and guidelines published between January 2020 and March 2026. Search terms included “anaphylaxis”, “pediatric anaphylaxis”, “adrenaline”, “epinephrine”, “autoinjector”, “intranasal adrenaline”, “food anaphylaxis”, “omalizumab”, and “oral immunotherapy”. International guidelines, consensus documents, systematic reviews, pharmacokinetic studies, and pediatric studies were prioritized. Food remains the leading trigger in children, but drug, Hymenoptera venom, cofactor-dependent, and non-IgE-mediated mechanisms must be systematically considered. Adrenaline is underused in community settings despite being the only life-saving drug. Intranasal adrenaline represents the most visible delivery innovation: it may reduce needle-related barriers and simplify administration, but current evidence is largely based on pharmacokinetic/pharmacodynamic studies and limited pediatric clinical data. Omalizumab and oral immunotherapy are reshaping long-term risk reduction in food allergy but do not remove the need for emergency adrenaline.Conclusion: The pragmatic management of anaphylaxis in children and adolescents entails self-management and hospital-based care. Intramuscular adrenaline is the first-line treatment when anaphylaxis is ongoing or recurrent, whereas adjunctive therapies should be considered on clinical grounds. Discharge recommendations should be individualized and include structured education, risk assessment, emergency planning and specialist follow-up. Intranasal adrenaline is a promising innovation, but its introduction requires clinical positioning, pharmacovigilance, cost-effectiveness evaluation, and continued emphasis on early treatment.
No comments:
Post a Comment