Abstract
Background
Respiratory syncytial virus (RSV) is the leading cause of lower respiratory tract infection (LRTI) in infants. Although influenza, parainfluenza, and human metapneumovirus also contribute to LRTI-related hospitalizations, their comparative population-level healthcare burden is not well defined. This study compared population-level healthcare utilization (HCU) associated with RSV-LRTI and LRTI caused by other respiratory viruses (ORspV-LRTI).
Methods
This nationwide retrospective cohort study used electronic health records from Clalit Health Services (CHS), covering more than 5 million individuals in Israel. Infants born in 2015–2023 and hospitalized before 12 months of age with PCR-confirmed viral LRTI during the RSV season were included. Acute healthcare utilization (HCU) was assessed within 30 days following hospital discharge, and long-term respiratory HCU was evaluated through 6 years of age.
HCU was expressed as population-level event rates per 100 000 live births during the study period, and incidence rate ratios (IRRs) were estimated using quasi-Poisson regression.Results
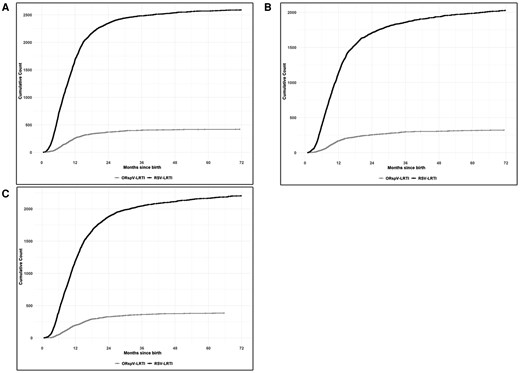 |
| Cumulative healthcare utilization through 6 years of age in children with RSV-LRTI and ORspV-LRTI. |
Conclusions
RSV-associated LRTI in infancy is associated with substantially greater population-level HCU than LRTI caused by other respiratory viruses, both acutely and throughout early childhood, supporting prioritization of early-life RSV prevention strategies.
No comments:
Post a Comment