Background
Methods
We enrolled a prospective cohort of all adult patients admitted to 2 academic hospitals in Vancouver, Canada with PCR-confirmed SARS-CoV-2 during the first wave of COVID between March and June 2020.
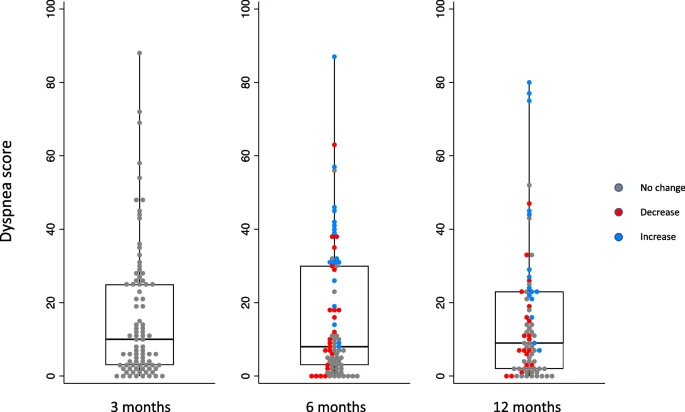
Dyspnea was measured 3, 6, and 12 months after initial symptom onset using the University of California San Diego Shortness of Breath Questionnaire.Results
A total of 76 patients were included. Clinically meaningful dyspnea (baseline score > 10 points) was present in 49% of patients at 3 months and 46% at 12 months following COVID-19. Between 3 and 12 months post-COVID-19, 24% patients had a clinically meaningful worsening in their dyspnea, 49% had no meaningful change, and 28% had a clinically meaningful improvement in their dyspnea. There was worse sleep, mood, quality of life, and frailty in patients with clinically meaningful dyspnea at 12 months post-COVID infection compared to patients without dyspnea. There was no difference in PFT findings, troponin, or BNP comparing patients with and without clinically meaningful dyspnea at 12 months. Severity of dyspnea and depressive symptoms at 3 months predicted severity of dyspnea at 12 months.
Conclusions
Post-COVID dyspnea is common, persistent, and negatively impacts quality of life. Mood abnormalities may play a causative role in post-COVID dyspnea in addition to potential cardiorespiratory abnormalities. Dyspnea and depression at initial follow-up predict longer-term post-COVID dyspnea, emphasizing that standardized dyspnea and mood assessment following COVID-19 may identify patients at high risk of post-COVID dyspnea and facilitating early and effective management.
No comments:
Post a Comment