- Research
- Open Access

Alhumaid S, Al Mutared KM, Al Alawi Z, et al. Allergy Asthma Clin Immunol. 2023 Aug 9;19(1):69.
Abstract
Background
Inborn errors of immunity (IEIs) are considered significant challenges for children with IEIs, their families, and their medical providers. Infections are the most common complication of IEIs and children can acquire coronavirus disease 2019 (COVID-19) even when protective measures are taken.
Objectives
To estimate the incidence of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection in children with IEIs and analyse the demographic parameters, clinical characteristics and treatment outcomes in children with IEIs with COVID-19 illness.
Methods
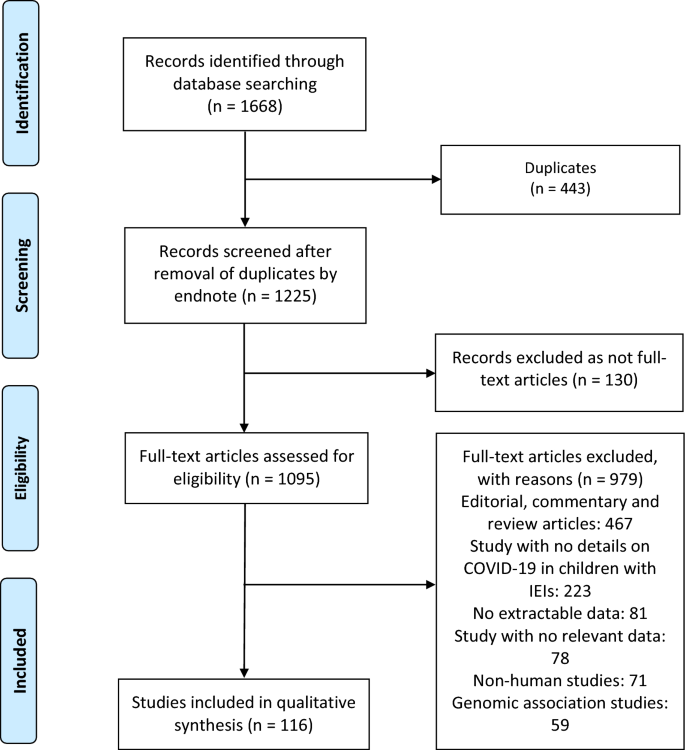
Results
Of the 1095 papers that were identified, 116 articles were included in the systematic review (73 case report, 38 cohort 4 case-series and 1 case–control studies). Studies involving 710 children with IEIs with confirmed COVID-19 were analyzed. Among all 710 IEIs pediatric cases who acquired SARS-CoV-2, some children were documented to be admitted to the intensive care unit (ICU) (n = 119, 16.8%), intubated and placed on mechanical ventilation (n = 87, 12.2%), suffered acute respiratory distress syndrome (n = 98, 13.8%) or died (n = 60, 8.4%). Overall, COVID-19 in children with different IEIs patents resulted in no or low severity of disease in more than 76% of all included cases (COVID-19 severity: asymptomatic = 105, mild = 351, or moderate = 88). The majority of children with IEIs received treatment for COVID-19 (n = 579, 81.5%). Multisystem inflammatory syndrome in children (MIS-C) due to COVID-19 in children with IEIs occurred in 103 (14.5%). Fatality in children with IEIs with COVID-19 was reported in any of the included IEIs categories for cellular and humoral immunodeficiencies (n = 19, 18.6%), immune dysregulatory diseases (n = 17, 17.9%), innate immunodeficiencies (n = 5, 10%), bone marrow failure (n = 1, 14.3%), complement deficiencies (n = 1, 9.1%), combined immunodeficiencies with associated or syndromic features (n = 7, 5.5%), phagocytic diseases (n = 3, 5.5%), autoinflammatory diseases (n = 2, 3%) and predominantly antibody deficiencies (n = 5, 2.5%). Mortality was COVID-19-related in a considerable number of children with IEIs (29/60, 48.3%). The highest ICU admission and fatality rates were observed in cases belonging to cellular and humoral immunodeficiencies (26.5% and 18.6%) and immune dysregulatory diseases (35.8% and 17.9%) groups, especially in children infected with SARS-CoV-2 who suffered severe combined immunodeficiency (28.6% and 23.8%), combined immunodeficiency (25% and 15%), familial hemophagocytic lymphohistiocytosis (40% and 20%), X-linked lymphoproliferative diseases-1 (75% and 75%) and X-linked lymphoproliferative diseases-2 (50% and 50%) compared to the other IEIs cases.
Conclusion
Children with IEIs infected with SARS-CoV-2 may experience higher rates of ICU admission and mortality in comparison with the immunocompetent pediatric populations. Underlying immune defects does seem to be independent risk factors for severe SARS-CoV-2 infection in children with IEIs, a number of children with SCID and CID were reported to have prolonged infections–though the number of patients is small–but especially immune dysregulation diseases (XLP1 and XLP2) and innate immunodeficiencies impairing type I interferon signalling (IFNAR1, IFNAR2 and TBK1).
No comments:
Post a Comment