
Abstract
Background
Our previous 2007 study reported a 19.4% rate of biphasic anaphylaxis in Kingston, Ontario. Since then, few updates have been published regarding the etiology and risk factors of biphasic anaphylaxis. This study aimed to describe the incidence of and predictors of biphasic anaphylaxis in a single centre through a retrospective evaluation of patients with diagnosed anaphylaxis.
Methods
From November 2015 to August 2017, all patients who presented to the emergency department at two hospital sites in Kingston given a diagnosis of “allergic reaction,” “anaphylaxis,” “drug allergy,” or “insect sting allergy,” were evaluated. Patients were contacted sometime after ED discharge to obtain consent and confirm symptoms and timing of the reaction.
A trained allergist determined if criteria for anaphylaxis were met and categorized the reactions as being uniphasic, biphasic, or non-anaphylactic biphasic. A full medical review of the event ensued, and each type of anaphylactic event was statistically compared.Results
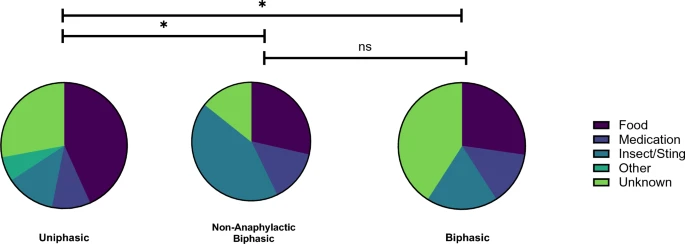 |
| Reaction profiles. The proportion of anaphylactic triggers across the responder groups is represented by pie charts. |
Conclusion
The incidence of biphasic reactions in this cohort was 15.94% and the average second-phase onset was 19.0 h. In biphasic reactivity, it appears that the symptom profile second reaction is less severe compared to the first reaction.
No comments:
Post a Comment